
CONTACT SPORTS
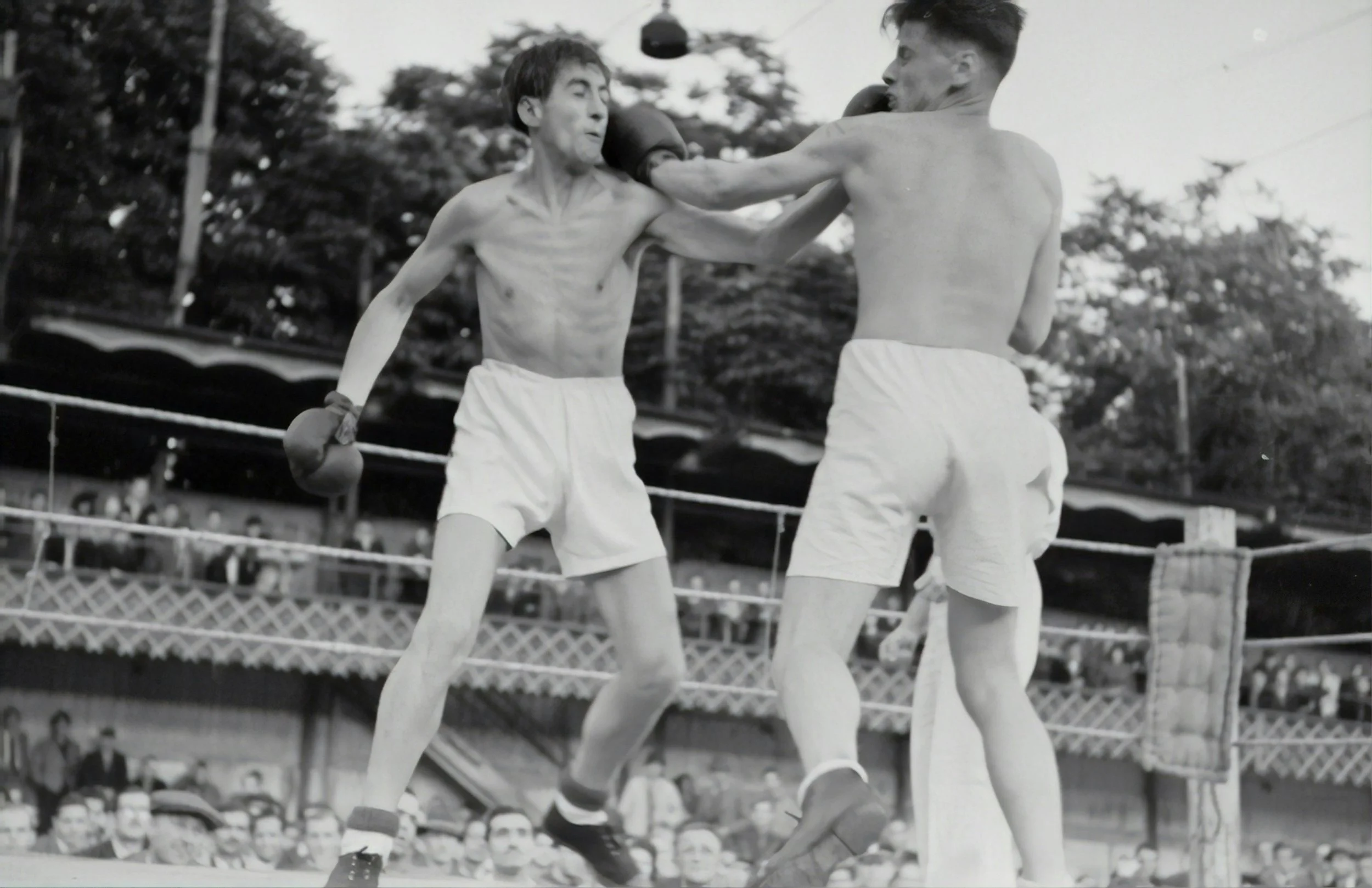
The world of contact sports is grappling with the ever present and increasing understanding that repetitive blows to the head, both sub-concussive and concussive, are linked to mood disorders in the short term and to longer term early onset brain degeneration in its multitude of forms from Chronic Traumatic Encephalopathy (CTE) , Parkinsons, Dementia and Motor Neurone Disease (MND).
Significant funding is now being directed towards research focused mainly on Concussion and Traumatic Brain Injury (TBI).
Some attention is being paid to the sub-concussive, mild repetitive traumas, such as heading a football or head locking in a scrum. Yet as Assistant Professor Bertrand Huber from CTE research centre in Boston reports: “The number of years of exposure to contact sports, not the number of concussions, is significantly associated with more severe tau pathology in CTE, suggesting that repetitive head trauma, including sub-concussive injury, is the primary driver of disease”.[i]
Even less attention (if any) is being paid to the housing of the brain – the skull and underlying membrane system. These structures are living tissue that have evolved specifically to absorb trauma in order to protect the brain, yet it is widely assumed that these structures are inert and that even the mildest of hits goes straight through the bone and membrane affecting only the brain. The experience of osteopaths in this field suggests otherwise.
The skull is made up of 22 individual bones that sit in positional relationships with one another – like a 3 dimensional jigsaw puzzle. These positional relationships can be disturbed by impacts of any time.
The underlying dural membrane system is a strong fascial system that holds a ‘tadpole’ shape. The dural membrane has what biologists term ‘tensegrity’. Architects and engineers also know about tensegrity. It is a feature of an arrangement of a material such that it can withstand forces by a distortion of its shape and when the forces subside it springs back into its original shape.

When a skull is subject to repetitive trauma, especially over years or maybe decades, this membrane structure will become overwhelmed and fatigued and eventually unable to spring back into its normal shape. The consequence will be a distortion in the shape of the compartments of the brain and potential interference with the blood and lymph drainage out of the cranial cavity. These are challenging circumstances for its occupant - the brain.
The concept of Membrain Disorder suggests how such a scenario can in the short term result in a change in the behaviour of the brain manifesting as a mood disorder, ranging from a low grade depression to even a full blown psychosis. If unresolved, long term this could be a predisposing factor for early onset brain degeneration.
An osteopath trained in the cranial field has a unique skill and is able to palpate (feel) the skull and underlying membrane system. Through this skilled palpation it is possible to tell if sutures (joins) between the individual bones of the skull are compressed and if there is distortion in the shape of the tadpole shaped dural membrane system. It is also possible to sense the quality of the membrane system and whether it is fatigued, agitated, chaotic or congested. In such circumstances a player would be diagnosed with suffering from Membrain Disorder and successfully treated.
Ideally all players of contact sports should be head checked at the end of each season and treated, if appropriate before the beginning of the next season.
All players who have retired should also be head checked.

A subset of the members of the osteopathic profession are setting up a ‘HANDS ON HEADS’ campaign to start to get this message across to the contact sports world. The campaign is starting with the care of some grass root rugby union club players. As well as diagnosing and treating the players, the plan is to initiate research on inter-practitioner reliability in diagnosing Membrain Disorder and further research on a players susceptibility to Membrain Disorder based on historic head trauma – right back to birth. Layers of historical head trauma not associated with contact sports are not being considered by the scientific world but this is of huge significance. If a player suffered a traumatic birth, for example, he or she may well have a plagiochephalic skull (a ‘crooked head’). An individual with a ‘crooked head’ is more likely to require an orthodontic intervention (they may have a cross bite or an over bite associated with the plagiocephaly). After the correction and the orthodontic braces come off, it is not uncommon for the dentist to fix wire retainers on their teeth. The concept of Membrain Health versus Membrain Disorder would propose that players with this history will be far less resilient to the same number and severity of blows than a player with a skull that is wide, symmetrical and sturdy. Research is needed.
The UK osteopathic profession is trailing behind the USA where early in 2025 a grant of more than two million US dollars was awarded to research the impact of cranial osteopathic manipulation on the treatment of TBI. Dr Gunnar Brolinson, sports osteopath and leading academic, is involved with this research alongside neuroscientist and biomedical colleagues based out of Virginia Tech University. [ii] [iii]
There are significant research papers emerging. The lymph drainage from the cranial cavity has been shown to be closely associated with the complex bony structure of the nose and nasopharynx.[iv] The question is, do the complex positional relationships of the nasal bones and cranial base play a role in hindering lymph drainage? An osteopath in this field would say yes. The geometrical shape of the brain has been shown to play a significant role in the behaviour of the brain.[v] The question here is does a distortion of the dural membrane system affect the geometric shape of the brain? An osteopath in this field would anticipate that it does.
If you are interested to explore this subject further – whether player, trainer, sports therapist or scientist- please get in contact.
[i] Huber,B., Stein,T.D., Alosco,M.L., Mckee,A.,(2017) Potential Long-Term Consequences of Concussive and Subconcussive Injury Phys Med Rehabil Clin N Am https://pmc.ncbi.nlm.nih.gov/articles/PMC4866819/ doi 10.1016/j.pmr.2015.12.007
[ii] Brolinson P.G et al (2022) Cranial manipulation affects cholinergic pathway gene expression in aged rats. J Osteopath Med; 122(2): 95–103
[iii] Brolinson P.G Osteopathy in the Cranial Field as a Method to Enhance Brain Injury Recovery: A Preliminary Study Neurotrauma Reports Volume 3.1, 2022 Neurotrauma Reports
DOI: 10.1089/neur.2022.0039
[iv] Jin-Hui,Y., Hokyung, J., Hae Jin, K. (2024) Nasopharyngeal lymphatic plexus is a hub for cerebrospinal fluid drainage https://www.nature.com/articles/s41586-023-06899-4
[v] https://www.nature.com/articles/s41598-020-78880-4
Geometric shape of the brain and its effect on its behaviour